
HAYLEY COULSON
Hayley Coulson is Physiotherapist at the Queensland Paediatric Haemophilia Treatment Centre, Lady Cilento Children’s Hospital, Brisbane

Hayley Coulson and Moana Harlen at the Congress
Photo: Hayley Coulson
The World Federation of Haemophilia Congress in Glasgow provided a great opportunity to listen to speakers from across the world. This report will briefly touch on some of the sessions I attended and found most valuable as a physiotherapist.
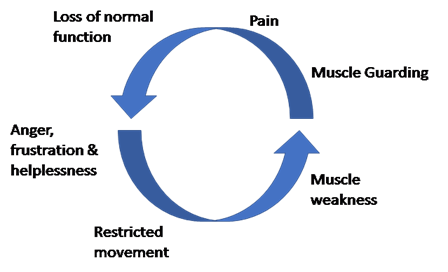
Plenary – Gaining insight into the complexity of pain in patients with haemophilia
Nathalie Roussel, Belgium
Roussel commenced her presentation with research studies showing that there was a high prevalence of pain in people with haemophilia. 85% of people with haemophilia had suffered pain in the last 6 months. 89% reported this interfered with their daily life. 50% indicated this was constant pain.
Roussel gave a very interesting overview of how pain works and some of the issues for people with haemophilia.
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage.
International Association for the study of pain
Abnormal pain physiology results in an overactive ascending pathway to the brain. This leads to critical levels of nerve excitement which can impact on the message to the brain (‘action potential’) and increase the pain response and decrease pain thresholds.
However, neuroplasticity (changes in the function, structure and biochemistry of the brain) can change the brain/pain cycle. Pain results in increased brain activity. Emotional responses such as stress, depression, worrying, fear of movement and hypervigilance should be considered when managing pain as a patient’s behaviour will impact on their recovery. If pain is impacting on an individual’s day-to-day activities, appropriate referrals and action needs to be taken to support this person in managing the pain as best as possible.
Education about pain is encouraged, and treating individuals need to be on the same page (psychologist, physiotherapist, doctors and nurses).
It is important to pay attention to the pain mechanisms and establish a proper treatment plan:
| Type of pain | Treatment approach |
| Nociceptive pain, i.e. pain arising from the stimulation of nerve cells (acute vs chronic). In haemophilia prior cause is tissue damage. | Medications? |
| Neuropathic pain: nerve related pain | Medications |
| Neuroplastic pain: pain is arising from the CNS (central nervous system) | Pain is not always a reliable signal. Medication |
Chairs: Nicholas Goddard, Angela Forsyth
Childhood
Manuel Carcao, Canada
This was my favourite presentation of the Congress. Dr Carcao focused on the importance of early presentation and treatment in joint bleeds. He discussed the mission to preserve joints from childhood to improve joint outcomes in adulthood. Children, whether they have haemophilia or not, are born with perfect joints. He discussed three case studies of severe patients with different outcomes:
| Bad outcome | Not a good outcome | Good outcome |
| 18-year-old male | 18-year-old male | 18-year-old male |
| Moved from another country where they used 'on-demand' therapy. Started prophylaxis late | Commenced prophylaxis early but had poor adherence | Commenced prophylaxis early, excellent adherence |
| Imaging reveals right elbow and right ankle damage with osteochondral (smooth surface at the end of bones) changes | Imaging reveals right knee, right ankle and left ankle changes with increased fluid and hemosiderin (a protein that stores iron in your body) deposits | Imaging showed no damage |
The place of ultrasound
Carlo Martinoli, Italy
Classification and difficulties of assessment
Horacio Caviglia, Argentina
Pitfalls
Sylvia Thomas, Brazil
Ultrasound is being used more across the world in many HTCs to review joint, synovium and cartilage changes in people with bleeding disorders. For the health care practitioners who use ultrasound in HTCs, this session covered some valuable technical issues relating to diagnosing.
Many discussions throughout the Congress recommended appropriate training in use of ultrasound to ensure effective diagnosis and avoiding the synovitis “mimickers”. This session discussed two mimickers in particular:
Ultrasound has been utilised as an effective assessment tool that is also inexpensive when compared to other methods of imaging. Ultrasound is recommended in combination with a comprehensive physical examination.
Overall the Congress for 2018 was informative with lots of new research arising from HTCs around the world. While there are breakthroughs with the utilisation of ultrasound in assessment, in other areas such as general bleed management, musculoskeletal assessment and outcome measures remain the same, with recommendations made for ongoing research into the most effective outcome measures for the bleeding disorder population.
I would like to thank Haemophilia Foundation Australia for the opportunity to attend the Glasgow Congress to not only learn about emerging changes in the management of haemophilia at an international level but also the opportunity to network with the bleeding disorders community.
Hayley Coulson was funded by HFA to represent the Australian and New Zealand Physiotherapy Haemophilia Group at the WFH 2018 World Congress.