
Jane Portnoy
Jane Portnoy is Social Worker – Haemophilia at The Alfred hospital, Melbourne
Chair: Moana Harlen
Youth Myth Busting was the most exciting session that I attended. I really enjoyed the energy and involvement from the audience.
The session involved three teams: a youth team, and adult team, and a health professional team. There were a series of ‘myths’ and the question was posed whether each myth was true or false. The audience voted, true or false, and then the teams were given a chance to answer and support their response. Finally the audience was asked if they had changed their views. There was a chance for comments and more questions, and we were really lucky to hear from so many members of the community about their own experience.
We were lulled into a sense of false security with a couple of easy ‘myths’ where there was a general consensus; these included ‘prophylaxis means that there are no more bleeding problems’ and ‘tattoos are perfectly safe for people with bleeding disorders’. However, the myths became more controversial, and there was a broad range of different views. The answers were rarely straightforward. Yes … but, or No … maybe, or perhaps! Or … but if you put it that way … seemed to be very common.
The most interesting thing for me was the stories that were told to support or to demonstrate a particular point. Talking about telling your boss about your bleeding disorder was one area where there were many examples on both sides. Generally it seems that being proactive and taking responsibility for yourself was really positive and successful way of approaching this area. However, we did hear of one young woman who was fired after she informed her manager of her haemophilia. She went to the union and was supported to approach her employer. She got her job back and the offending manager was dismissed.
Another interesting debate was ‘it is inappropriate to discuss sex and bleeds with your treating team’. Of course, this seemed obvious to me, but then one of the young people said it was really uncomfortable as he had known his treating team his whole life, and it felt a bit like talking to your auntie about sex … YUK! It seems that whilst the professionals are in agreement that this it is appropriate and reasonable to talk sex and bleeds, usually they don’t bring these things up. So it’s left to the patients. One of the great strategies we heard about was the session at the ‘blood brothers camp’ where anonymous questions are able to be put to either one of the haematologists or the nurses. Usually a great conversation follows; of course everyone wants to know about the same things.
Thanks to Hannah, who worked hard to put this session together before she left HFA for a new job.
Chair: Cameron Cramey
Understanding pain … in 20 minutes!! – Martina Egan-Moog
Evolving concepts in pain management – A/Prof Carolyn Arnold
Clinical application of modern pain sciences for People with Bleeding Disorders (PWBD), an ‘active approach’ – Catherine Pollard
I found the Pain Management session to be really helpful. Of course there are many tried and tested strategies of pain management, and for many people these work well.
It is always beneficial to listen to pain specialists speak about how they work with pain, what is helpful, and what are some of the challenges. Dr Arnold was, as always, insightful about how to manage pain. She emphasized that whilst medication is a part of the story, other strategies are also very important. Some other strategies were then talked about by the speakers who followed.
Catherine Pollard, haemophilia physiotherapist in Auckland, spoke about using the gradual physiotherapy approach, making sure to avoid the boom and bust cycle, which does lead to reduced functionality. Catherine described a very gradual increase in exercise with close supervision of a physiotherapist which enabled a person with a bleeding disorder to return to their previous level of functioning; whilst a too fast approach led to further injury and slowed down the recovery process.
Have you heard of DIMs and SIMs? Martina Egan-Moog presented a really useful idea. Martina talked about how our body has danger and safety receptors not pain receptors. The more our sense of safety is the lesser our need for a protective pain response. DIMS stands for Danger in me: anything that is dangerous to your body tissues, life, lifestyle, job, happiness, your day to day function. Essentially anything that is a threat to who you are as a person. SIMS are Safety in Me: anything that that makes you stronger, better, healthier, more confident, more sure and certain within and about yourself.
The diagram below explains how these both can modulate our pain experience.
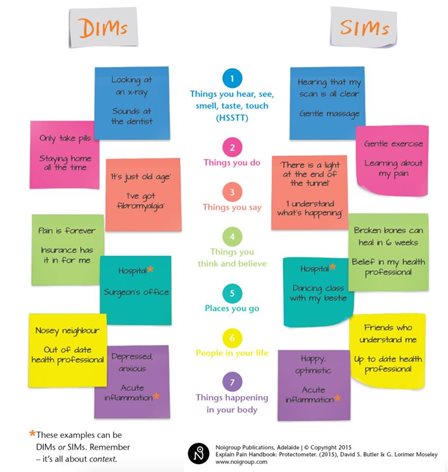
Diagram reproduced with permission from Noigroup Publications
Chair: Dr Jenny Curnow
Let’s Talk Period: Women and bleeding disorders – Dr Paula James
Panel Discussion: Dr Jenny Curnow, Dr Chris Barnes, Dr Paula James, Dr Dominic Pepperell
Dr James spoke about women and bleeding disorders and how often bleeding disorders in women can go undiagnosed. Her Self-BAT (self-administered bleeding assessment tool), which is on her Let’s Talk Period website (letstalkperiod.ca), was developed to help concerned women to better understand whether their bleeding episodes are normal or abnormal.
Interestingly she spoke about how stress levels can affect your factor VIII levels. In extreme circumstances they can double or even triple them. This can lead to difficulties in VWD testing and discrepant results. In the panel discussion, the haematologists spoke about the reluctance from the medical field to label a person with a specific disorder if doctors are uncertain of the diagnosis, but they also acknowledged that this doesn’t diminish the person’s bleeding experience and that these women still require treatment to manage their bleeding.
Chair: Dan Credazzi
Why do we use MyABDR? – Dr Chris Barnes
Working with the community – Suzanne O’Callaghan.
A HTC Royal Children’s Melbourne experience – Julia Ekert
MyABDR in the clinic and at home:
Paediatric – Dr Chris Barnes and Karan
Adult – Andrew Atkins and Michael
Moving Forward with MyABDR – Dr Chris Barnes
I thought that the session on why to use MYABDR was greatly enhanced by the patient and family stories of how they had used this method of reporting bleeds and treatments. They described frustrations and system limitations; however, MYABDR has improved greatly and most of the glitches are gone. When they do have a problem the MyABDR Support team is really helpful. One thing that was only briefly touched on was the desire of the young adult to rebel and with a chronic illness such as a bleeding disorder the rebellion can have lifelong effects. I think that talking about this system is incredibly important and hearing about the frustrations is equally vital.