
It is an exciting time with more new haemophilia treatments likely to become available in Australia, but there have been a lot of questions about them and what they will mean for treatment and care. How do they work? What difference will they make for people with haemophilia? How will they impact on comprehensive care?

In the New therapies webinar for Bleeding Disorders Awareness Month, Dr Liane Khoo and Dr Sally Campbell gave simple and clear presentations explaining the new extended half-life (EHL), non-factor therapies and gene therapies for haemophilia and were joined by haemophilia nurse Stephen Matthews for a Q&A to answer audience questions.
HFA Zoom and Facebook Live webinar,
13 October 2022
Facilitator ~ Natashia Coco, Haemophilia Foundation Australia
Speakers
~ Dr Liane Khoo, haematologist & Director, Haemophilia Treatment Centre, Royal Prince Alfred Hospital, Sydney
~ Dr Sally Campbell, haematologist & Acting Director, Queensland Haemophilia Centre, Royal Brisbane & Women’s Hospital
~ Stephen Matthews, Clinical Nurse Consultant, Haemophilia Treatment Centre, Royal Prince Alfred Hospital, Sydney
~ Sharon Caris, HFA Executive Director
Watch the webinar online
Understanding the way haemophilia treatments work can be challenging and Dr Liane Khoo’s presentation on newer haemophilia therapies was a very user-friendly explanation of the sophisticated technologies involved.
She explained that the definition of prophylaxis has changed in recent years. It now covers ‘the administration of agents’ – it is no longer limited to infusing clotting factors into a vein but can be a range of therapies given in a variety of ways. The goal of prophyaxis is also more ambitious – aiming to prevent bleeding, allowing people with haemophilia ‘to lead active lives and achieve comparable quality of life’ to people who do not have haemophilia.
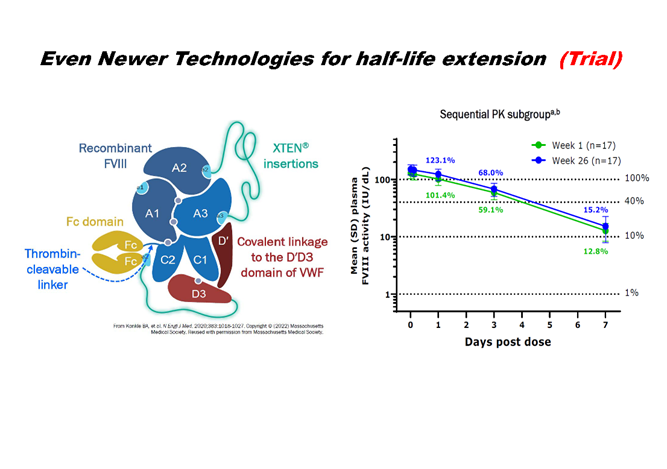
Adding the sugar molecule PEG (polyethelene glycol) to haemophilia replacement factor therapies has meant that their half-life can be extended, ie, how long it takes the active substance in factor to reduce by half in the body. As a result, the factor lasts longer in the body and fewer injections are needed.
Other ways of making the factor last longer in the body have been by attaching other types of molecules to it, such as fusion proteins. There are now also clinical trials of even newer technologies to extend the half-life of factor, with good results.
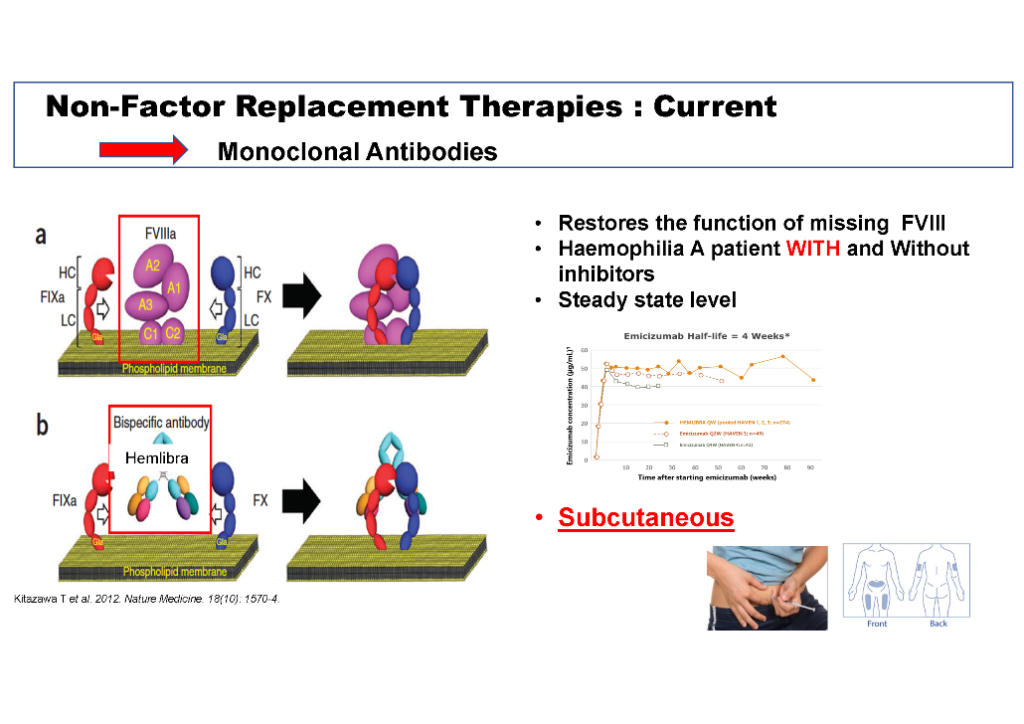
Liane Khoo explained that monoclonal antibodies like Hemlibra® (emicizumab) do the same job as factor VIII (8) by helping the body to form a clot. However, these treatments work a bit differently to replacement factor therapy:
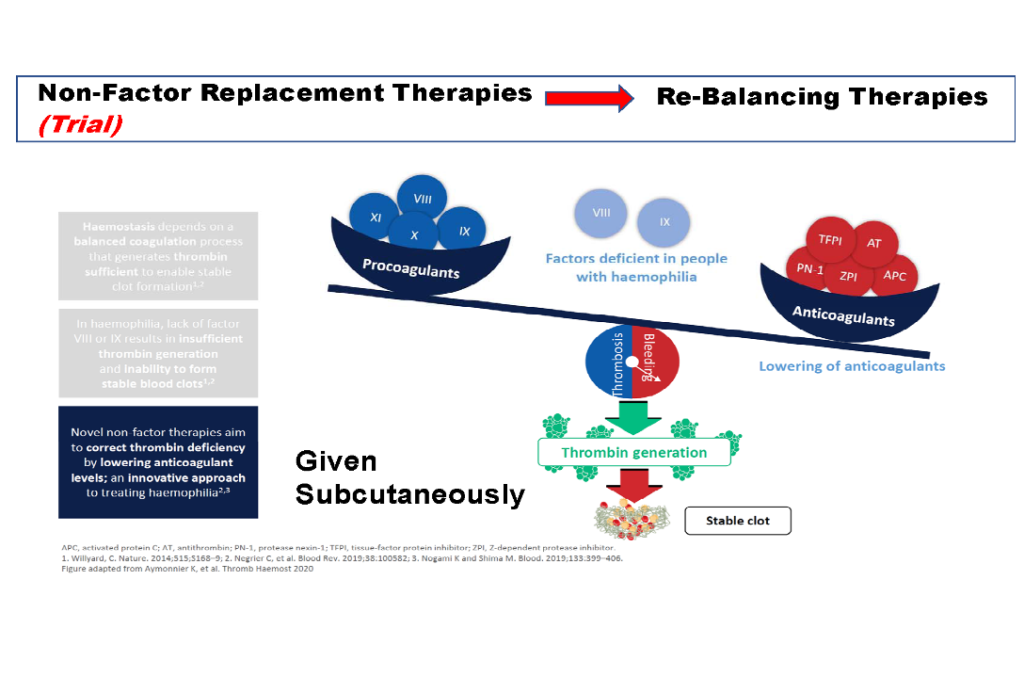
She also touched on rebalancing therapies that are currently in clinical trial. These therapies are different again. They work by lowering anticoagulants to balance the deficiencies in clotting factors VIII (8) or IX (9) that cause haemophilia.
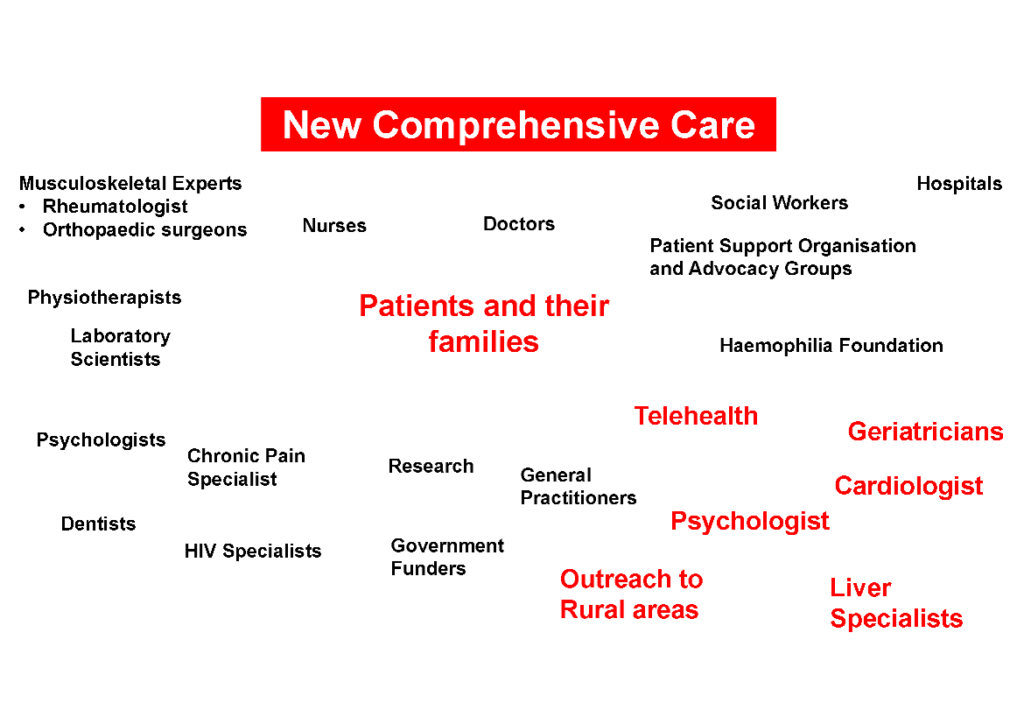
What do these new therapies mean for comprehensive care? She looked at the situation when the patient and their family is at the centre of care and the multiple services that would need to be available across Australia, no matter where you live, to achieve the goals of care.
Dr Sally Campbell introduced her presentation with a list of the haemophilia treatments currently available in Australia and commented that with individualized treatment, each person with haemophilia would need a treatment that is right for them – and that what is right for one person may not be for another.
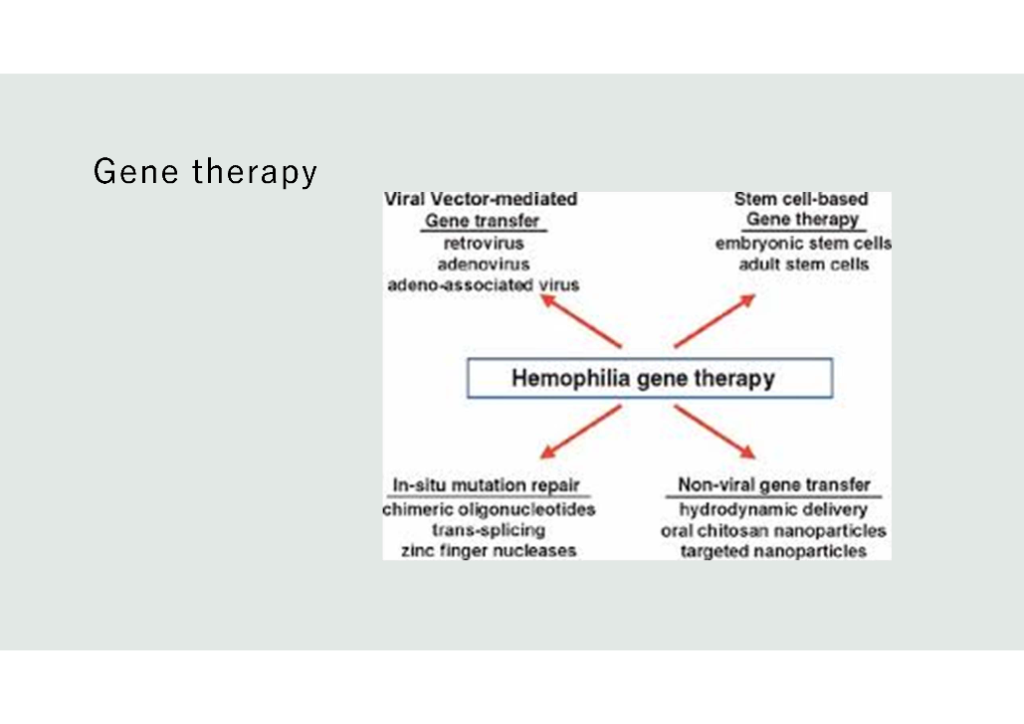
She focused on gene therapy for haemophilia. Viral vector-mediated gene transfer is now in advanced clinical trials, but three other approaches to gene therapy are also being explored: stem cell-based gene therapy, in-situ mutation repair and non-viral gene transfer (see the slide below). She explained briefly how the different types of gene therapy work and, in particular, the viral vector-mediated gene transfer method in haemophilia.
She explained that the medicines review processes have just commenced for haemophilia gene therapies in Australia and that they will take some time before gene therapies are available to patients. Patient considerations for gene therapy will include:
It will be important to discuss these questions with your Haemophilia Treatment Centre team, but liver health will be a key issue, as all of the current AAV gene therapies target the liver. She pointed out that what would be classified as a ‘success’ with gene therapy would be very individual and depend on what you wanted to achieve with the treatment.
Stephen Matthews and Sharon Caris joined Liane Khoo and Sally Campbell to answer questions from the audience.

What would gene therapy for haemophilia involve for a patient?
If I have had hep C and been cured, can I have gene therapy?
What are the timeframes for access to gene therapy in Australia?
What can I do to prepare myself for gene therapy?
Discussion also highlighted that people can consider new therapies and see some benefits even if they are older and have damaged joints.
This was a lively and informative webinar – many thanks to the speakers for putting it together.