
SUZANNE O’CALLAGHAN
Suzanne O’Callaghan is HFA Policy Research and Education Manager
VWD
Chair ~ Dr Chee Wee Tan
Personal story ~Adam
Personal story ~ Susie
VWD diagnosis ~ Dr Geoffrey Kershaw
VWD clinical management ~ Dr Nalini Pati
The von Willebrand disease (VWD) session began with Adam’s story of his personal journey with type 3 VWD. He has always been very physically active, but as he has grown older, he has become more aware of the impact of bleeds from injuries on his long-term health, as well as experiencing gastrointestinal bleeds, and is now looking at ways to manage this better into the future. He has learned to self-infuse and has considered employment options to support working from home to help manage bleeds. His advice to others with VWD:
He finished with the comment that VWD is a disorder, not a disease – a view held by many in our community.
Susie followed with her experiences of living with type 1 VWD. Susie’s story is published separately in this issue of National Haemophilia.

Diagnosing VWD is complex and specialised. Dr Geoffrey Kershaw gave a remarkably accessible presentation on the key aspects of laboratory testing in an area that is very scientific. He explained that different regions of the von Willebrand factor (VWF) structure have different functions: binding to collagen or FVIII (factor 8) or platelets through glycoprotein 1b (Gp1b). These different functions relate to the laboratory tests available.
Testing and results can be affected by many variables. For example, an individual’s VWF levels can increase because of stress, physical exertion and inflammatory illnesses and the sample must be kept at a specific temperature range for its quality to be maintained.
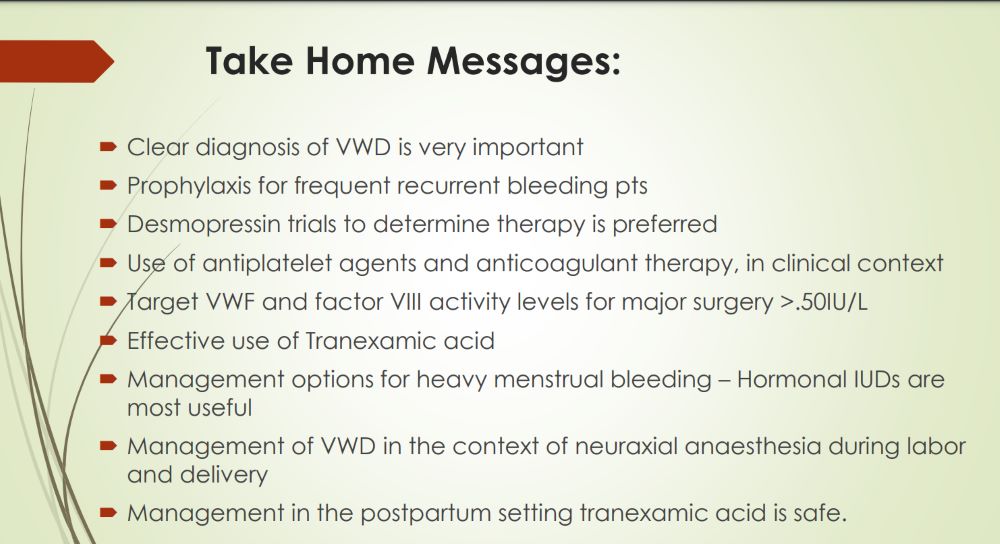
In a presentation on the medical issues, Dr Nalini Pati highlighted some of the factors affecting a patient’s journey to appropriate diagnosis and treatment.
A lack of awareness among general practitioners and other health professionals in the wider community and a wide variation in presentation means that VWD diagnosis often occurs late. He noted that treatment needs to be personalised but that treatment options in Australia are currently limited.
There was a consensus in the session that current challenges include:
This was discussed in the final plenary, with a recommendation from Assoc Prof Chris Barnes that VWD needs to be included in the Australian Bleeding Disorders Registry (ABDR), along with education of health professionals in the wider community.